
- Slug: BC-CNS Tapachula Migrant Health, 3,030 words.
- 9 photos and captions below.
By Laura Bargfeld
Cronkite Borderlands Project
TAPACHULA, Mexico – On a cool Monday morning in early March, dozens of people – migrants and citizens alike – line up outside a public health clinic as rush hour traffic hums by.
One man’s knee is wrapped. Another has a large growth on his face. A teenager is pregnant. Mothers and fathers hold coughing babies, some parents cough themselves. A child vomits onto a pink cloth on a woman’s shoulder.
As she waits, Karla Matute, 35, holds the right hand of her son, Joryí, 7, whose left hand is wrapped in thin gauze at the wrist. They are migrants from Honduras.
When Matute gets to the front of the line, she shows the nurse a letter from the Mexican government’s refugee agency, known as COMAR, giving her permission to seek free treatment for her son. She says someone from the Red Cross told her that he may have a fractured arm.
They came to the clinic, Matute said, after a public Tapachula hospital told her they could not treat Joryí for free because she hadn’t started the asylum application process and they aren’t Mexican citizens.
Public directories list more than a dozen hospitals in Tapachula – but depending on interpretation of law and policy by hospital staff – some turn migrants away if they can’t pay, others only treat them after a referral from a primary care clinic, and others only after they have paperwork proving they are in the asylum system. The situation is confusing for migrants seeking care.
The nurse asks, “Where do you live? I need your proof of address so that you can pass through to consultation.”
“Parque Bicentenario,” Matute replies, referring to a park in the city center where she and her son sleep in a tent.
The nurse looks up, confused.
“In the park?”
After further discussion, Matute and Joryí are allowed inside.
Health care in Tapachula was not built for this moment. It is a city of 350,000 in one of Mexico’s poorest, most under-resourced states. Tens of thousands of migrants heading north are stuck here as they await asylum meetings, humanitarian visas and other documents that will allow them to gain residency or legally continue their journeys to Mexico’s border with the United States.
And as policies enacted by Mexico and the U.S. have trapped migrants in Tapachula for months at a time, the city’s health care system has been entirely overwhelmed. The crush comes in addition to the ongoing effects of the pandemic, limited amounts of medication, the high costs of medical testing, paperwork inefficiencies and reports of discrimination based on race and nationality.
But experts say the situation in Tapachula would be far more dire without the involvement and dedication of nonprofits, nongovernmental organizations, and local health officials.
Under Mexico’s complex health care system, the law guarantees that all people, citizens or not, have access to basic care. That care is provided by a complex web of coverage that includes private insurers (for those who can afford it), employee-provided coverage, and various public coverage programs. But migrants can’t always access care, say experts and advocates. Communication between policymakers and providers on how to cover migrants and under which programs has been slow and unclear.
Underlying these challenges is the inability of Tapachula’s health care system to meet the needs of its own citizens. Medical providers face resource shortages and structural challenges brought on by limited government funding. Chiapas state has a poverty rate that far exceeds that of other Mexican states; almost 70% of the state’s population qualified for free public health care in 2020, according to Mexico’s Government Institute of Statistics and Geography.
Migrants, particularly women, children and those with chronic conditions, are among the most vulnerable to these gaps and disparities.
‘They threw them in the trash’
When Erliwe Germain went into labor in September, she had been sleeping in Tapachula’s Central Park for five days. Hungry and tired, and unable to find housing, she made her way to the public hospital, an experience she described as difficult and scary.
Germain gave birth in a room with seven other mothers. They didn’t even clean the baby, she said, only giving one unidentified injection and no followup care.
Germain had arrived in Tapachula with her husband, Dimitry Docile, just a few weeks before that. The couple, who are from Haiti, had been living in Chile, but she said they were subjected to racism there and wanted better for their unborn daughter. They migrated north and eventually made their way to Tapachula.
Having a baby in Tapachula has allowed Germain to get permanent residency status in Mexico, which affords her access to more services. Germain’s cousin, Christela Saint-Louis, and her cousin’s husband, Dieulifoute Dorme, are not so lucky.
Saint-Louis said her year-old son was born in Chile before the family started the journey to Tapachula with Germain. She suffers from ongoing medical issues that have gotten worse on the trek north.
Although UNHCR, the U.N. agency for refugees, claims they should be able to seek care and gave them the paperwork to do so, Saint-Louis said, they haven’t gotten the help they need.
In Haiti, Saint-Louis said, doctors operated to remove fluid in her lungs, and she had ongoing medical care after migrating to Chile. However, after walking through the Darién jungle from Colombia to Panama for five days, her breathing problems started again. She said she has lost weight and the pills she was given at a clinic in Tapachula, an antibiotic and anti-inflammatories, don’t work for her.
Dorme, who developed a rash on the journey, said the antifungal ointment he was given didn’t work either. Their children are well-prioritized by local organizations, he and Saint-Louis said, but in their experience, care for the adults is minimal.
Leila Castro came to Tapachula in March with her 7-month-old girl and 4-year-old son. They were dropped off at the shelter Jesús El Buen Pastor by immigration officials. Castro left behind two more children in Honduras.
One recent night, Castro’s daughter developed diarrhea, and then a rash on one shoulder. Castro said the doctor and nurse on staff at the shelter gave her electrolytes for the diarrhea but had no medication to treat the rash.
As the baby coughed, Castro held her tightly. The girl has a lung condition, and her health already is complicated, Castro said, but she intends to keep trying to find treatment for her daughter.
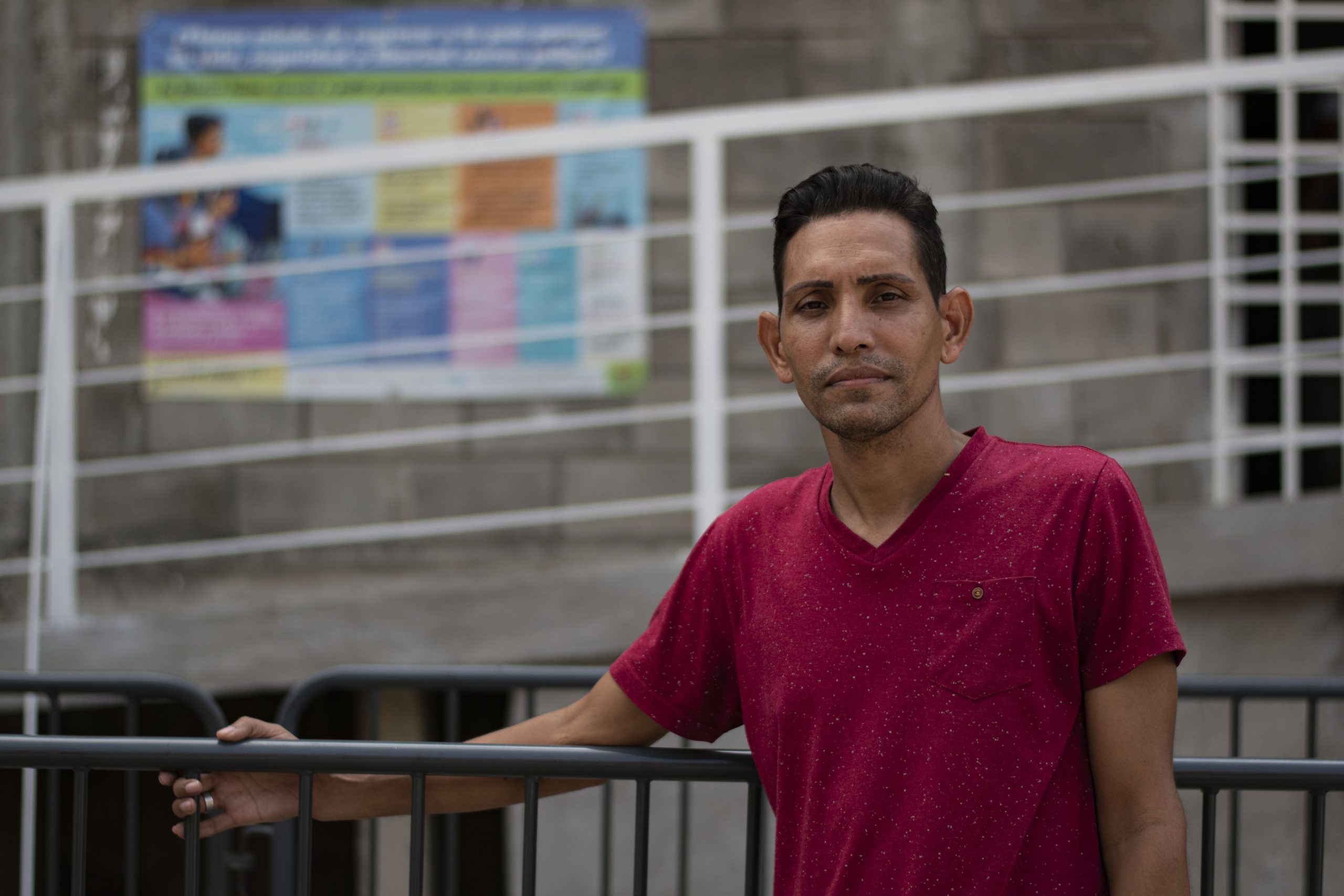
Roberto Báez Castillo was detained by immigration authorities just a day after arriving in Tapachula in late February. He was taken to Siglo XXI, the city’s immigration detention center, where he remained for 11 days.
When he got there, he said, he showed officials the prescriptions for his three-month supply of antiretroviral medication, which he’d received for free in Panama to treat HIV. But the paperwork didn’t matter, said Báez, who has been living with HIV for 12 years.
“These are all the documents I gave them so they would know I have my condition. And yet my medications were thrown away at Siglo XXI,” he said. “They threw them in the trash.”
As he waited outside the COMAR office, he recalled his long struggle with getting the medication he needs to manage his condition.
Báez, who is gay, said he fled Cuba to escape ongoing, violent discrimination from authorities. He spent a year in Peru without medication. Eventually, he made his way north to Panama City, where he finally started getting medical care in mid-2019.
On this day, he spoke with someone at the UNHCR office in Tapachula who told Báez the agency would connect him with a local nonprofit that serves HIV patients. It’s progress, but he remained distressed that it could be another week before he would get antiretrovirals, putting him at further risk for complications from the virus.
‘Not as bad as it was’
To understand how so many gaps in access exist for Tapachula’s migrant population, it’s necessary to look at the complex network of available care.
The vast majority of primary health care for migrants is provided by NGOs – nonprofit, nongovernmental organizations – including shelters, many of which are still reeling from the huge increase in migration over the past few years and the effects of the pandemic.
“Nothing here is enough,” said Laura Benitez, the project manager for Global Response Management’s site in Tapachula. Among other things, the international NGO provides free medical services in Tapachula on a walk-up basis. No paperwork is necessary.
Benitez, who also has experience working with migrants in Tijuana, said things have been especially difficult in Tapachula since 2019, when U.S. demands that Mexico slow northward migration led Mexico City to institute a containment policy for migrants who entered the country from Guatemala. The previously transient population became a static one, overwhelming health and aid workers.
“The health system collapsed, basically,” Benitez said, “and there’s not many NGOs. If we compare this with Tijuana, it’s like, we don’t have enough.”
Global Response Management addresses a need among migrants for good primary care they can easily access. The agency recently moved its office from a public clinic to a park complex called Tapachula Station, where other services, including dentistry, are available. Workers treat such issues as dehydration, foot injuries, fevers and skin conditions.
The team of fewer than 10 serves 20 to 50 people a day, and Benitez predicts those numbers will increase as word of their new location spreads.
“I’m sure in a few weeks, we’ll have more patients,” she said.
Paperwork has been a major barrier for migrants seeking medical care, Benitez said. When migrants apply for asylum in Tapachula, their first point of contact is with the COMAR office to get an appointment date and time. At that appointment, they receive official documents that allow them to more easily access services, including health care at public clinics and hospitals.
However, Benitez said, at the end of 2021, asylum seekers were receiving appointments as far as six months out, causing delays for those with urgent health needs.
“In six months, they cannot work, they cannot leave, they don’t have money, they don’t have food to eat, and they don’t have access to medical health services because they don’t have the document,” she said. “So it was desperate times. It was chaos.”
Although wait times have improved, COMAR staff members still are overwhelmed as the flow of asylum seekers into the city continues.
“People were coming to us crying. They didn’t know what to do,” Benitez said, “but now it’s better. It’s not OK, but it’s not as bad as it was.”
Paperwork, however, is just one hurdle. Haitian and African migrants in particular face shortages of interpreters in medical settings, as well as widespread reports of systemic racism and anti-immigrant bias.
“It’s not just about them being migrants,” Benitez said. “It’s about them being dark-skinned.”
Research by Amnesty International and the Haitian Bridge Alliance released in October contained accounts from Black migrants in Tapachula of “intersecting forms of discrimination in accessing health care, based on language, race and nationality.”
And one 2020 study from the Population Council in Mexico about migrant women’s access to reproductive health care in Tapachula found that discrimination and racism has a measurable effect and “acts to the detriment of these women’s health.”
Female migrants of multiple ethnicities have reported physical reactions to this discrimination, the study said, including “high blood pressure, tachycardias and stress and anxiety symptoms.”
Although the report highlighted efforts to hire Haitian migrants as interpreters and translators, the researchers made it clear these resources aren’t sufficient.
‘There’s a magic word’
Dr. David Jiménez, coordinator of attention to the migrant population in Sanitary District VII of the Ministry of Health of Chiapas, is a big believer in order.
Every day, he reviews data sent to him by COMAR and other agencies. Jiménez is responsible for 108 health units – clinics, hospitals and ambulances – in Tapachula and the vicinity. There are services in each of the shelters, too. As he spoke, he answered multiple calls requesting ambulances and medical services from around the city. In essence, everyone in Tapachula answers to him when it comes to the government response to migrant health care.
“There’s a magic word,” Jiménez said. “It’s called teamwork.”
Although the health system as a whole faces challenges, Jiménez cited many ways in which the state health ministry has been successful in working with such NGOs as UNHCR and UNICEF to facilitate medical care for migrants in Tapachula.
UNHCR has donated ambulances, masks, gloves and auxiliary ventilators to medical settings in Tapachula and throughout the region. It also has provided access to prenatal ultrasounds and support for newborns.
Additionally, UNHCR works with the local university to make more interpreters for Haitian migrants available and makes pamphlets and banners in Spanish and Creole that provide instructions on preventive health care and how to seek services.
“And these materials also benefit the entire population, because it is material that everyone needs, not only refugees and migrants,” said Pierre-Marc René, a public information associate for UNHCR Mexico.
UNICEF also is filling gaps in maternal health care by hiring a gynecologist and providing resources to support children, adolescents and pregnant women. It serves about 150 patients a week, according to a UNICEF report from mid-March.
Lastly, with assistance from the federal programs IMSS-Bienestar and Grupo Beta, Jiménez and his team have assured that most every shelter in Tapachula has some level of medical staffing and transport to hospitals when necessary.
Despite these steps, some gaps remain.
Herbert Bermudez, a worker at Albergue Jesús El Buen Pastor, said he sometimes uses his own money to buy medicine for migrants who can’t find what they need in the shelter’s supply of donated medications.
In addition, COVID-19 continues to be a challenge in many shelters, creating staffing shortages and safety concerns because of overcrowding, which forced some to shut down, UNICEF reported in late March.
Jiménez acknowledged that it was difficult at the beginning to treat so many people from so many cultures, but said they’ve come a long way.
“I do not think I know perfection, but I think that we are already getting to know each person: the migrants from different countries,” he said.
But he also expressed long standing frustrations.
In his experience, Jiménez said, Haitians in particular are constantly in conflict with those who’re trying to help them, always pushing to the front of the line. He wants everyone to follow the system laid out for them and go through proper channels.
Jiménez also said migrants prioritize their health after everything else, especially immigration appointments and their attempts to leave Tapachula.
“More than anything, you need to know how the migrant puts other things first,” he said. “The least important of those things is their health.”
Benitez at Global Response Management also spoke to this phenomenon, although with a differing perspective.
“There’s a lot of people who need medical attention or psychological help, but they have other priorities,” she said. “Even if they know they need it (medical care), they prefer to go look for a job or make money to feed their family.”
More support needed
President Andrés Manuel López Obrador (referred to as AMLO) addressed the inefficiencies in this web of health care in a large-scale reform of Mexico’s health care system in early 2020. Healthcare reform was a major talking point of his campaign in 2018.
Although the strengths and weaknesses of the old system, known as Seguro Popular, were nuanced, it did guarantee asylum seekers three months of free health care access once they had their asylum appointments.
AMLO’s government created a fully public option, known as INSABI, to make health care more accessible for all, including migrants. Public funding was expanded by 35% in 2020 to meet these goals. That ended the three month limit for asylum seekers and expanded access, on paper anyway.
But communications about policy and expectation remain poor, according to some medical researchers, and there are widespread accounts of medication shortages and access issues for migrants and Mexican citizens alike. In addition, there have been reports of corruption within hospitals, which, when supplies are low, may charge patients for resources that should be free.
Experts also have criticized López Obrador for severely underfunding health care. An independent analysis in 2020 indicated health care in Mexico is under-resourced by as much as 658.5 billion pesos. And despite some funding increases, that gap hasn’t been closed.
Although the Chiapas health ministry contributes resources for migrants, the majority of the funding Jiménez distributes comes from NGOs. Jiménez is proud of the strides his team has made, but more support is needed, he said.
Jiménez said the NGOs he works closely with would soon be petitioning AMLO, who visited Tapachula on March 11, asking that “more resources be allocated to the health system.”
Benitez agreed that resources from the Mexican government have been lacking.
“The government doesn’t do enough,” she said. “That’s why it’s important that we NGOs are here.”
Government reforms have also been affected by the ongoing pandemic. Mexican public hospitals, which serve people who need more than basic care, often have found themselves overwhelmed, and wait times in emergency rooms remain high.
Furthermore, private and specialized treatment is beyond the financial reach of many migrants.
Caught in these currents are migrants like Karla Matute, the Honduran mother who sought help for her son’s injured arm.
At the clinic, a doctor put a more durable wrap on Joryí’s arm and referred him for an X-ray at the local hospital. Matute said the arm likely isn’t broken – Joryí would be in more pain if it were – but it’s worth checking to be sure.
They left the clinic with painkillers, but instead of heading to the hospital, Matute went to the National Immigration Office (INM). The night before, she had heard the agency might be giving humanitarian visas to the single mothers with children who’ve been sleeping in the park.
For the moment, anyway, Joryí’s arm will have to wait.
She’s hoping to leave soon and make her way north to Monterrey, where she heard there is work.
Additional reporting was contributed by Jennifer Sawhney, Juliette Rihl and Salma Reyes. Translations were done by Jennifer Sawhney and Salma Reyes.
For more stories from Cronkite News, visit cronkitenews.azpbs.org.
^__=




(Photo by Juliette Rihl/Cronkite Borderlands Project)



